1. Aeromedical Problems

Photo:
Iver Søndergaard
Pressure conditions
The average passenger airliner cruises at an altitude of approximately 30.000-36.000 ft., equivalent to 10-12 km. The outside pressure at this altitude is about ¼ atm (atmosphere) or 190 mm Hg (fig. 1).
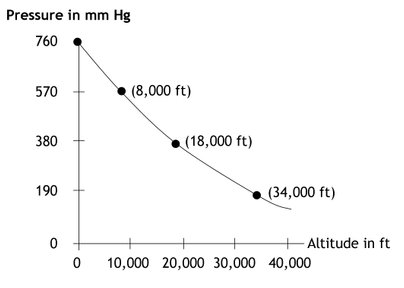
Fig.1.
Relationship between altitude in ft.
and pressure in mm Hg.
These days, all civil airliners are equipped with a so-called pressurized cabin. Compressors maintain a difference in pressure between the cabin and the outside atmosphere. At the normal cruising altitude the cabin pressure corresponds to 6-8,000 ft. (3/4 atm). Pressure wise this corresponds to the passengers be situated on a mountain at a height of 2.000-2.500 m. In new types of planes the pressure will be reduced less. In these planes the pressure is corresponding as being in an altitude of 1.800 m.
Cruising altitude is usually reached within 10 to 15 minutes of take-off and descent will begin approx. 30 minutes before landing. During short flights lasting 30-40 min the plane only reaches a cruising altitude about 5-6 km, and the cabin pressure will be reduced correspondingly.
At normal cruising altitude with a cabin pressure of ¾ atm. trapped air will try expanding 38%.
Thus trapped air in the bowel will lead to a more distended abdomen. In more serious cases air can be trapped elsewhere e.g. intracranial where an expansion of air can lead increased pressure on the brain.
Due to these conditions some patient with e.g. intracranial air, untreated pneumothorax, or larger subcutaneous emphysema should not be transported using commercial flights. Are such patients to be transported by air, it has to be done at a cabin pressure of 1 atm corresponding to sea level. If an airplane is to maintain a cabin pressure of 1 atm. it can fly at a maximal altitude of 5-8 km depending on the construction of the plane. In such cases air ambulances are used.
Oxygen pressure and hypoxia
The composition of the atmosphere remains very constant up to extremely high altitudes. Its most important constituent elements are nitrogen (79%) and oxygen (21%).
At sea level the alveolar partial pressure of oxygen is 103 mm Hg and it falls linearly to an altitude of approx. 10,000 ft. corresponding 3,3km. At this point hyperventilation takes effect and deflects the linear progression. Moreover, 10,000 ft. is the highest permitted flying altitude without an oxygen supply, unless the aircraft cabin is pressurized. The alveolar partial pressure of oxygen at this height is 60 mm. Hg/8 kPa (fig. 2).
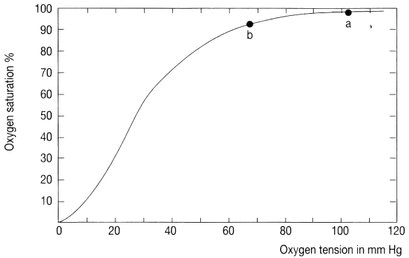
Besides the partial pressure of oxygen, the blood’s oxygen bearing capacity plays a part in oxygen supply to the critical tissues - above all the brain and the heart. Fig. 3 shows the hemoglobin-oxygen dissociation curve for a normal person with a normal hemoglobin concentration. At sea level the blood is almost fully saturated with an oxygen saturation of 97-100%. At normal cruising altitude with a cabin pressure at ¾ atm. the oxygen saturation has decreased to approx. 92-94%.
This will not cause the average healthy passenger any problems, but can do so in the case of the passenger suffering a cardio-pulmonary disease or anemia. Conditions causing an increased metabolism e.g. fever lead to an increase in the demand of oxygen and in general patients suffering from fever should not fly.
As previously mentioned in new types of planes the cabin pressure is reduced less, which leads to higher oxygenation – and oxygen saturation – in cruising altitude.
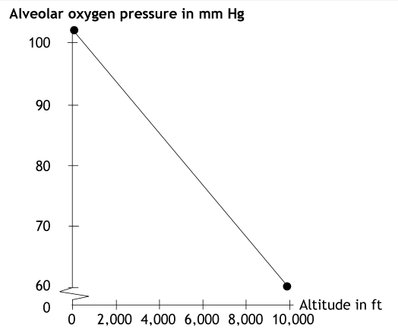
Fig. 2.
Relationship between altitude in ft. and alveolar partial oxygen-pressure in mm Hg.
Besides the partial pressure of oxygen, the blood’s oxygen bearing capacity plays a part in oxygen supply to the critical tissues - above all the brain and the heart. Fig. 3 shows the hemoglobin-oxygen dissociation curve for a normal person with a normal hemoglobin concentration. At sea level the blood is almost fully saturated with an oxygen saturation of 97-100%. At normal cruising altitude with a cabin pressure at ¾ atm. the oxygen saturation has decreased to approx. 92-94%.
This will not cause the average healthy passenger any problems, but can do so in the case of the passenger suffering a cardio-pulmonary disease or anemia. Conditions causing an increased metabolism e.g. fever lead to an increase in the demand of oxygen and in general patients suffering from fever should not fly.
As previously mentioned in new types of planes the cabin pressure is reduced less, which leads to higher oxygenation – and oxygen saturation – in cruising altitude.
001. Frontpage
001. Foreword
001. Contributors
001. Aeromedical Problems
012. Planning the Air Transportation of Patients
013. Airline Requirements
015. Transportation of Disabled Persons
016. Cardiac Disorders
019. Gastrointestinal Disorders
010. Central Nervous System Disorders
011. Ear, Nose, and Throat Disorders
012. Eye Disorders
013. Mental Disorders
014. Gynaecological and Pregnancy Problems
015. Transportation of Sick Children
016. Infectious Diseases
017. Orthopaedic Injuries
018. Cancer
120. Acute Mountain and Decompression Sickness
021. Burns and Plastic Surgical Problems
122. Airsickness
123. Jet Lag
124. The STEP System
125. Specialised Transportation of Patients
126. First Aid on Board – Legal Considerations
27. The History of Air Transportation of Patients
28. Oxygen supplementation in flight - a summary
Latest update: 19 - 09 - 2022
Accelerations
Normally the effect of an ordinary airliner’s acceleration on passengers is without importance.
As regards the positioning of patients, it is usual to place the head facing the direction of flight because the impact of the acceleration at take-off is greater than the one of the deceleration during landing. Due to these reasons patients with increased intracranial pressure must be positioned with their head facing the nose of the plane. (These patients should also only be transported by air ambulance at a cabin pressure of 1 atm).
Vibration, noise and turbulence
The effects of vibration, noise and turbulence are generally much less in a jet aircraft than in a propeller driven aircraft. Flight altitude and speed are also of vital importance as turbulence is usually greater the lower one flies and at low speed. For this reason jet rather than propeller driven air transport is to be preferred for long distance flights. Propeller driven aircraft may be used for short flights, and have the advantage of being able to land on smaller airfields should this be necessary.
Helicopter transportation enjoys the great advantage of being able to carry patients almost directly between hospital and airport. This can save both time and a difficult journey over bad roads, mountains, etc. On the other hand, helicopters are noisy, and subject to vibration and shaking. The cabin pressure is appox. 1 atm which is an advantage to some patients. More and more helicopter ambulances are used for primary evacuation taking patients straight from the site of damage to hospital.
Humidity
The humidity is low in the cabin. The relative humidity is low, as the pressurized cabin air is from 10 km altitude, heated from approx. – 50° C to cabin temperature. The humidity does not reach 0 because it is being mixed with a fraction of the recirculating air having already been humidified by the passengers.
The low humidity often gives rise to irritation of the mucous membranes - especially of the eyes and airways creating a particular risk for patients having had surgery performed recently in these areas.
Risk of venous thromboembolism
When passengers during long flights are sitting being immobile in a seat for many hours, stasis occurs in the deep veins of the lower leg. This is a cofactor in developing deep venous thrombosis (DVT).
The risk of developing a DVT is very small though it is increased at flight lasting longer than 4 hours and also if the passenger has other risk factors for developing a DVT.
As dehydration is also a cofactor in developing a DVT, it is very important to drink plenty during a flight. Having a diuretic effect alcohol and coffee should be consumed with caution.
Sleeping pills can cause a long period of immobilization why especially passengers with risk factors for developing DVT are advised against such use.
Knee-length graduated compression stockings have proven to have an effect in preventing development of DVT on long distance flights and at the same time they also prevent edema in the lower legs, which a lot of passengers suffer from during a flight.
General advices when flying:
Stay as active as possible during the flight. Going for a short walk every hour and moving your feet frequently when seated are recommended. Drink plenty - but alcohol and coffee should be consumed with caution. Avoid the use of sleeping pills. More and more airline companies have information with exercises one should be doing during the flight.
If prior to the flight having other risk factor for developing a DVT, one should when travelling flights with a duration of more than 4 hours consider the following guidelines while still keeping the general advices in mind:
Conditions causing minor increased risk
Age over 40
Larger varicose veins
Obesity (BMI>30)
Recent laparoscopic surgery
Recent bed rest (>3 days)
Recommendations: No prophylaxis is needed. Optionally graduated compression stockings.
Conditions causing moderate increased risk
Previous DVT
Late pregnancy/ first weeks of postnatal period
Moderate congestive heart failure
Severe respiratory conditions such as cold
Severe infectious diseases during the last couple of weeks
Blood diseases or conditions causing an increase in coagulation
Treatment with estrogen including birth control pills
Lower leg surgery including knee arthroscopy
Recommendations: Graduated compression stockings.
Conditions causing high risk
Major fractures in leg or pelvic region
Major traumas especially pelvic
Recent hip or knee alloplastic surgery
Recent major surgery
Malignancy especially during chemotherapy
Blood diseases or conditions causing a severe increase in coagulation
Severe congestive heart failure
Previous pulmonary embolus
Recommendations: Graduated compression stockings plus prophylaxis with low molecular heparin (LMWH) injected subcutaneously 2-4 hours before the flight. Obviously this should only be given if the patient is not receiving actual anticoagulant treatment.
People with more than one risk factor should be evaluated individually.
E.g. a passenger being late pregnant, or just haven given birth, and who previously have suffered from a DVT, should be moved from the moderate risk category to the high risk group and hereby be given LMWH. Likewise can a flight lasting longer than 8 hours change the risk profile for an elderly immobile passenger from e.g. low to moderate.
THE RECOMMENDATIONS WRITTEN ABOVE ARE ONLY INTENDED AS A GUIDE AND IF ANY QUESTIONS OF DOUBT CONCERNING PROPHYLAXIS ONE SCHOULD ALWAYS CONSULT THE TREATING DOCTOR.
Acetylsalicylic acid has not proven to have an effect in preventing DVT.
In the future rivaroxaban, which can be prescribed as tablets, will probably be used in the way, we use LMWH today. The drug though cannot be used by pregnant.
Fig. 3.
Haemoglobin-oxygen dissociation curve for a normal adult at 37o C and pH 7,4.
a: Oxygen saturation at sea level.
b: Oxygen saturation at cabin pressure in normal cruising altitude.